
I’m In The Vulnerable Class for COVID-19. A Plea To Take This Virus Seriously. |  |
| I’m In The Vulnerable Class for COVID-19. A Plea To Take This Virus Seriously. Posted: 12 Mar 2020 02:22 PM PDT A friend of mine recently texted me in a fury. “Someone just posted on FB that we’re doing things to stop the virus only because it’s going to ‘hurt old people’s feelings’ if we don’t,” he said. His mother has respiratory issues and thus falls into the “older person vulnerable to the new coronavirus” category, as do many others. Like me. And I can read. So when I read tweets or posts about how it’s basically “just a flu” (false) that “only hurts the vulnerable,” it makes me worry for us as a society. If we can’t protect our most vulnerable, what are we doing?
COVID-19: We Need to Consider Society As a WholeI’ve received many reader emails about COVID-19 asking for my thoughts given that I am currently dealing with a cerebrospinal fluid (CSF) leak and an inflammatory immune condition that already predisposes me to medication reactions and a cytokine storm. It’s been very surreal to see the news unfold at a time when I have been in quarantine of sorts (bedrest) for many, many months. Due to the CSF leak, I rely on family and friends for groceries and to make food as I cannot do so myself. For those who are chronically ill, the lack of independence for basic needs adds an extra layer of concern and need for care on a daily basis. The discourse about COVID-19 seems to consist of differing responses from several distinct groups of people First, the people who are well and who believe they’ll be unscathed. This “isn’t a big deal,” they say. “Why is the media making us panic?” Second, those who are vulnerable like me, and who know they are at risk for significant complications if they contract the virus. There are some people who live in between those two extremes, and while healthy themselves are nonetheless able to remember a series of subclasses whose lives legitimately depend on the collective to stay safe. And then, there are others whose actions are downright dangerous for all of us. This includes NBA player Rudy Gobert. Per Hot Air’s report:
After mocking COVID-19 precautions by touching a bunch of things, he then tested positive. And as with any exponentially spreading virus, this exposure and infection have predictably led to others testing positive.
Ultimately, Engel isn’t wrong from a statistical perspective. He’s also not the first or last person I’ve seen try to stem the panic by reminding people of the expendability of the vulnerable like me. I’m writing this post as a plea to each person to put overall societal needs above individual desires until this virus peaks and subsides. I am not a doctor, and the following is not medical advice. It is, however, a summary of what I’ve researched for my own safety given my risk levels due to the issues with my immune system Disinformation and panic don’t help anyone, especially during a pandemic.By now, you’re probably living under a rock if your’e unaware of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the artist formerly known as 2019-nCoV until it was named COVID-19. People also refer to it as "coronavirus", but since it’s one of many coronaviruses, I’m not going to do that here. People also refer to it as the "Wuhan flu,” but since it’s actually not a flu virus and people are already erroneously comparing it to the flu, I’m going to stick to COVID-19 for this piece. (See below for my response to the the “it’s just the flu” people.) COVID-19 is a called Novel Coronavirus because it’s a new disease for humans. The World Health Organization estimates a global death rate of 3.4% of those who are infected. While many people around the world may have built up immunity to various flu strains over time, the newness of COVID-19 means no one had immunity to it when it first broke out. There is also no established treatment for COVID-19, and there is presently no way to cure it. The fast spread of this virus has led to heavy amounts of disinformation and even outright conspiracy theories. I’ve argued with quite a few people online who suggest that this is “just like the flu,” or that “most people barely feel sick.” In an internet age where we are able to quickly get data from countries that are ahead of our curve here in North America, there is simply no excuse for not acting as swiftly as possible. Panic isn’t useful. Changing nothing in your life isn’t useful either. It’s actually outright dangerous right now. In the middle lies being informed, prepared, and willing to think about society as a whole. Doing so lowers the burden on our health care systems, and buys a bit more time for treatments and research to happen. Reducing the number of people who are sick at once is the best way to keep our health system from being overwhelmed. And that in turn helps not just COVID-19 patients but also everyone else who must seek treatment in a hospital. Two factors that make COVID-19 a big concern to everyone:
Yes, the bulk of infections will be mild. Those people will still transmit this highly contagious disease, though. And even if you’re fully asymptomatic, you can still spread this virus as a vector. Which is why acting now, even if you’re healthy, is critical. This also means preparing without panic, being reasonable about what we need and don’t need without hoarding, and above all considering our roles as citizens in a collective. As Mark Manson said in a new post:
Or, as Dr. David Juurlink, a physician at Toronto's Sunnybrook Health Sciences Centre, says, “The faster this hits us, the less able we will be to provide care. The less able we are to provide care, the more people will die. It is as simple as that." This chart put together today by the Institute of Disease Prevention shows the potential mitigation of COVID-19 for King and Snohomish counties in Washington State by taking precautions sooner rather than later.  Infections with and without social distancing COVID-19, courtesy of the Institute for Disease Prevention This virus is beyond containment worldwide, and acting swiftly but calmly is imperative. Learning from ItalyOutside of mainland China, Italy now has the highest number of deaths in the world from COVID-19. And the country's fatality rate from COVID-19—at 5%—is much higher than the global average of 3.4%.
Why is Italy’s death rate so high? Italy has conducted a substantial number of tests — more than 42,000 as of Saturday (March 7), according to Al Jazeera. But the size of the outbreak and the late adoption of containment measures combined with speed of spread meant that Lombardy and to a lesser extent other areas in Italy are unable to get back to a place of balance. The strain on the system is so bad that the Italian College of Anesthesia, Analgesia, Resuscitation and Intensive Care (SIAARTI) has shared guidelines (link is in Italian) for the criteria that doctors and nurses should follow in these extraordinary circumstances, likening them to the moral choices doctors face during wartime. They require doctors to allocate ICU access to the patients with the highest chance of therapeutic success. This may seem logical and even utilitarian, but it’s a devastating position to be in every day during an outbreak. At the same time, an Italian doctor begged other countries to act now. Dr. Daniele Macchini posted (link is in Italian; English here) about what’s happening on the front lines of Italian’s coronavirus response, noting that each ventilator was like gold and that many of the doctors were themselves getting sick with the virus. He notes that there are no more specialist doctors, just doctors as a whole, a single team to try and stop the inflow of sick people. Italy does have a sizeable older population, but the case study of Dr Macchini and others on the front lines would be foolish to ignore. The foregoing is not “media hype” but rather published testimony and guidelines from a country right in the middle of a substantial outbreak. We need to think through the exponential growth of this disease, and we don’t seem to be doing so on a systemic level. The way exponential growth works is that it seems tolerable until suddenly it’s an avalanche – and then it’s often too late. Let’s try to avoid the avalanche. Risk Groups for COVID-19Briefly, because we’ve all been bombarded with graphs these days, a note about mortality and risk groups. The pre-existing conditions that are known to be factors in worsening COVID-19 infections in patients: 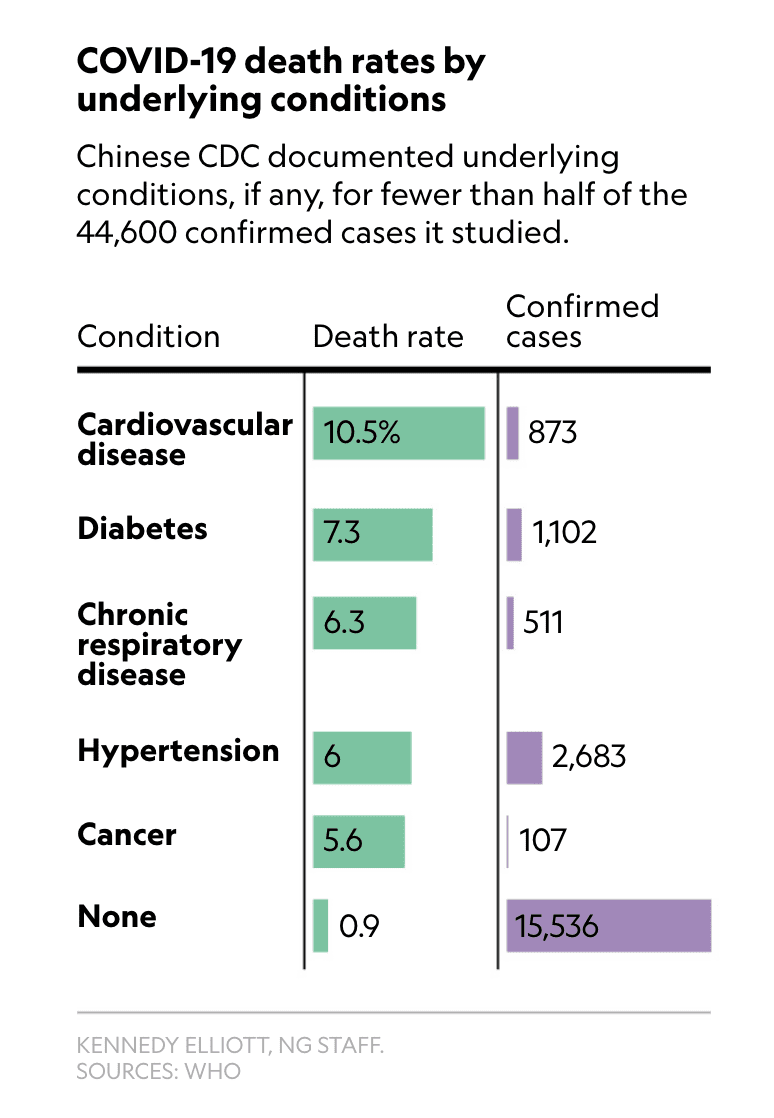 Risk factors COVID-19 via NatGeo The medical consensus is that those over 60 years old, and those with certain underlying health conditions, are most at risk. In addition to the main pre-existing conditions listed above, immunocompromised patients are at higher risk for fatalities. And there are millions of immunocompromised people in America alone, a number which not only comprises those with immunodeficiency syndromes but also people with cancer (who are accounted for in the above chart), or who have been treated for it, people who have received transplants, people with HIV, and more. For those who fall in the vulnerable class of patients, extra precaution is needed. What is also needed — as this post will keep saying over and over — is for everyone to take social distancing seriously, especially because of testing limitations in many countries but especially the United States. Symptoms and mitigation when starting to feel sickThe symptoms of Covid-19 vary from case to case. From China’s data, the most common are:
If you have a fever and dry cough alone, advice from interviewed doctors is to get tested by calling your department of health – NOT by presenting to the ER or Urgent Care where you could potentially infect others.
Generally, contacting your department of health for your state, province, or territory is the best option.
Where testing comes inData from Italy suggests that many cases went undetected and enabled community spread. This data is part of why it is extremely important to get testing capacity up to population numbers, and why containment in the USA is going to be a big problem. As of March 11, 2020, it’s still difficult to get tested in the USA. Several Legal Nomads readers in the USA have reported symptoms consistent with COVID-19, obtained doctors’ requests for testing, and still were told by the Departments of Health in their states that they were not eligible for testing. Those readers did the smart thing and put themselves on self-quarantine, but what of the many potentially infected people who did not?
Strain on the hospital system when catastrophe medicine is at play, especially in the USAThe facts for the US health care system during this pandemic are not great. According to the American Hospital Association, as of 2017, the US had 924,107 beds total. On a per capita basis, that was 2.77 beds per 1000 people. For comparison, China’s 2017 per capita bed ratio was 4.05 beds per 1000 people. (See OECD healthhcare stats here.) Put simply, there are not enough hospital beds in the USA for an outbreak of the kind we’ve seen elsewhere, nor for the projection of hospitalizations – 4 to 8 million – that researchers estimate the United States will see. In fact, the US's ratio of hospital beds per 1000 people is also smaller than those of the other main countries overwhelmed with outbreaks of this virus. The respective ratios for Italy and South Korea as of 2017 were 3.18 and 12.27. Moreover, with at-will employment in many states and many employees receiving few sick days — especially in jobs that are front-facing (service industry, food industry, etc.) — increased community spread is likely. And then there are patients who are chronically ill and depend on medication and hospital needs even outside the “at-risk” aspect of COVID-19. If the system is overwhelmed as we’ve seen happen elsewhere, deaths from pre-existing conditions that can’t get properly treated are more likely. From a family friend, a doctor in Indiana who reviewed the Indiana State Department of Health Crisis Standard for Ventilator Allocation:
Oh come on, isn’t it just like the flu?No. For the love of all things holy, NO. This isn’t the flu – it’s a different virus altogether. Scientists in Asia have described it as a cross between SARS and AIDS in terms of how it impacts the body. It is more contagious than the flu. It is more deadly than the flu. Even assuming a global death rate of 1% (despite the current rate of 3.4-3.5% of infected people per the WHO), it would be 10 times more deadly than the flu, which has a death rate of 0.1%.  COVID-19 vs the flu, courtesy of Bloomberg. The data from all around the world indicates a much higher mortality rate and a very different virus altogether from seasonal influenza. China’s datasets, as well as those from countries like Taiwan and Singapore where so far containment has been possible, have all provided us with information to help us see what’s coming. People who are usually reasonable and rational are nonetheless comparing this virus erroneously to the flu or saying it’s just overblown hype. This is not only unkind, to belittle someone’s fears about their own health and safety, but negligent for the wellness of society. Please don’t make fun of people who are scared of this very real threat, especially if they’re in the vulnerable class. Please don’t downplay actual data and case reports from around the world where doctors have been fighting this virus to the point of exhaustion. The success of our outcome depends on individual willingness to mitigate risk moment to moment. So what can we do? Think collectively, not individually, to help flatten the curve of the epidemic.
Those who require hospitalization require the long term stays of ICU care that I mentioned earlier, for a period of 3-6 weeks. Italy thus far estimates that many COVID-19 patients need at least 4 weeks on mechanical ventilators. That number would put hospital systems over capacity very quickly if we don’t flatten the curve on this virus. :no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19780273/flattening_the_curve_final.jpg "An infographic that shows the goals of mitigation during an outbreak with two curves. The X-axis represents the number of daily cases and they Y-axis represents the amount of time since the first case. The first curve represents the number of cases when no protective measures during an outbreak are implemented and displays a large peak. The second curve is much lower, representing a much smaller rise in the number of cases if protective measures are implemented.") via Vox news This virus is going to affect your life. And you get to decide if you want to contribute to flattening the curve, or spiking it. I sound like a broken record for social distancing because we know testing isn’t going to get everyone and thus if we want to have a bell curve more like South Korea versus like Italy, we need to start taking action on an individual level yesterday. I realize not everyone has the privilege to work from home or to take all the measures I list below. But doing as much as possible is extremely important for EVERYONE, in order to help ease the impact of this pandemic Fine, you’ve convinced me. Now how do I help stop the spread for COVID-19?Starting place: do not panic. Each of us thinks better and makes smarter decisions when we are not in cognitive overload. The earlier you take precautions, even if you’re not directly impacted yet by the virus, the better you can help lower the societal burden. Choose compassion for the societal burden over fear and distrust. I know it’s not easy, but as a collective we do depend on it. Worldwide data shows there is no advantage to being a late mover here. 1. SOCIAL DISTANCINGDoes your company let you work from home? Start doing so now. Limit nonessential public gatherings. Make small choices that can take out away from groups of people, even in quotidian activities. Refrain from museums, clubs, dancing, religious services, and more as this plays out. Crowded spots are prime dissemination spots. What is a “public gathering”? Doctors I have spoken with define a public gathering as anything more than 6 people, but there doesn’t seem to be consensus overall as you can see with the number (5) below. Regardless of the actual numbers, social distancing is how we can have a hope at slowing the spread of COVID-19, and potentially mitigate its effects on the hospital system. The same doctor in Indiana who wrote about ventilator allocation above, says:
This also includes cancelling non-critical medical visits, to keep the hospitals and systems as clear as possible for the coming burden. Telemedicine has been available for a few years now, and this is definitely the time to avail yourself of it if you have the privilege to do so. I’ve been telling people, “be St. Louis, not Philadelphia,” because in 1918, Philly held a huge parade during an influenza outbreak. In contrast, St. Louis cancelled all gatherings. As you can see from the chart below, the death toll was very different in those two cities.
It’s selfish to complain about “changing your plans” or making adjustments to social activity when the downside of doing nothing is systemic overload and catastrophe medicine. It should go without saying, but do NOT fly on a plane if you’re awaiting COVID-19 results. A passenger from New York to West Palm Beach, Florida did just that. Again, this isn’t hype, this is simply a summary of what we’ve seen in other countries to date with medical systems that don’t have enough beds for contagion at this volume. People like me don’t have the privilege to be out in the world safely right now, and nor do your parents and grandparents. WASH YOUR HANDS. OFTEN. LONGER THAN YOU WANT TO.The most important thing other than social distancing is to wash your hands, for 20 seconds. That’s a lot longer than most of us are accustomed to taking when we wash our hands. And we need to do it frequently. Before and after eating food. When returning home from outside. When in contact with anyone else. If there is a chance your unwashed fingers have the virus on them, you do not want them anywhere near you or your home. “Happy Birthday” sung twice is about the right length, so many people are singing that as they wash. Here’s a song generator from The Verge that can help you choose other options so you don’t hate birthdays by the end of this COVID-19 pandemic.
Soap works very well on this virus, and it doesn’t need to be anti-bacterial soap. It just needs to be a looooong wash, because of the nature of the virus. For the science behind why that is, see the thread below:
If you cannot use soap and water because you’re away from access to them, alcohol-based hand sanitizer with over 60% alcohol content is a good stand in. When you do get access to soap and water, though, wash immediately. STOP TOUCHING YOUR FACETHIS IS SO HARD. I’m not alone; a study from 2015 shows people touch their faces an average of 23 times per hour. It’s very important though, and we have to keep avoiding it as much as possible. This includes the eyes, since ocular transmission has been one of the ways the virus is spread.
DISPOSABLE GLOVES IN CERTAIN SITUATIONS.Wear nitrile or latex disposable gloves when in public spaces like buses, subways, and other areas where you will be touching areas that others have touched like pumping gas. If you are in a social situation where you need to remove your gloves, do not touch your face or eyes, no matter how much something itches. And before you put gloves back on, wash your hands thoroughly with soap and warm water, scrubbing the fingers. If you don’t have gloves but are using light switches, elevators, or other public buttons or switches, use your elbow to hit the button instead of your hand. STAY 2m (6 FT) AWAY FROM SICK PEOPLE, AND TRY TO KEEP DISTANCE OF 1m (3 FT) GENERALLY WHEN OUTSIDE.This means life changes that have irritated some people, but nonetheless are reasonable precautions during an outbreak like this. And still, social distancing takes precedence. Netflix instead of a movie theatre. If you’re want to dine out, there are ways to keep distance. Either get take-out food and bring it home, or sit outside if there is a terrace instead of staying inside a closed restaurant. You get the drill. THIS MEANS NO HAND SHAKING OR CHEEK KISSING TO GREET PEOPLE.Curtsy, arm pump, touch your feet together, it doesn’t matter as long as you’re not actually touching your hand or face to someone else’s hand or face. AVOID PUBLIC TRANSPORTATION AS MUCH AS YOU CAN.This likely doesn’t require an explanation, but is to avoid a cough, sneeze, or hand-to-hand contact that can put us in the danger zone for droplet splatter or air particles that can transmit the virus. DOORKNOBS: LEARN TO CLEAN THEM OFTEN AND TRY NOT TO USE THEM IN PUBLIC.I’m very limited here because of my CSF leak, but for those of you who can open and close doors using your elbows, hips, or shoulders: do it. If not, wear gloves to turn a doorknob, or wash your hands immediately after touching it. If someone does get sick in your household, wiping down your doorknobs is a good idea too. The CDC has a list of cleaning recommendations for COVID-19 here. WIPE DOWN YOUR CELL PHONE WHEN YOU RETURN HOME FROM OUTSIDE.I use alcohol-wipes for this, small size, but the ones I bought are no longer available. A spray bottle with rubbing alcohol sprayed onto a wipe will usually suffice. Apple used to say not to clean phones this way, but due to COVID-19, Apple has changed its guidelines. The company now says you can use a wipe with 70% isopropyl alcohol or a Clorox wipe to clean your iPhones. For non-Apple devices, see this piece from CNET. WHEN THE WEATHER ALLOWS, OPEN A WINDOW.This virus cannot linger in a well-ventilated space, per this FP article, though it’s quite cold in much of North America still. ON MASKSThere is a lot of controversy about masks. If you do choose to use one, you need to don and doff it with gloves on, and then make sure you properly dispose of the gloves. When the mask has been taken off, place it inside of a disposable container or bag, seal it, and put it in the trash. In a March 12th piece, The Guardian recommends wearing masks when caring for sick people and when around sick people:
If someone is coughing or sneezing it’s good to ask them to put on a mask to protect you. DON’T FORGET TO STAY SOCIAL, EVEN INSIDEI’ve been on bedrest now for close to two years, and with technology I’ve been able to keep myself sane and connected with friends. In times like this, where fear often takes over, it’s even more important to stay in touch with people you love even if you can’t see them. An epidemic of loneliness is not what does the immune system good. These are three things that really helped me during bedrest and isolation the last few years:
STOCK UP, RESPONSIBLYMake a list of crucial prescription medication as well as over-the-counter medication such as and cold/pain relief, and stock up for a month’s extra supply – or more if your insurance allows. In Canada, most people I’ve spoken with have gotten 2 months’ extra supply of prescription medication when they refilled their prescriptions. In the USA, this will vary by state and insurance provider. Other things to have in the house:
Some non-perishables that are easy to have in case you want to minimize your food trips: rice, canned tuna or chicken, protein bars, popcorn, crackers, nutritious seeds like flax or chia, peanut butter, oats, cans of chickpeas and beans, and oils you use to cook with. Also some frozen veggies. Don’t forget the pets! Stock up on pet food for an extra month. The vulnerable are worthy of protection too.On March 12th, Norway instituted a mandatory quarantine for all inbound travelers and cancelled classes at all schools, as well as all sporting events. They also have a mandatory quarantine for people coming into the country from abroad. In the USA and Canada, many of these large-scale domestic measures have not happened yet, though more and more cancellations are happening each day. We know that the countries that have been most successful at lowering their overall death rate are the ones that take swift, aggressive measures quickly. In South Korea, for example, nearly 20,000 people are being tested every day for the virus and labs are working 24/7 to get testing kits processed. This morning, I heard a segment on NPR from a man there who tested positive despite his only symptom being a slight cough. In Seoul, the radio anchor reported drive-through testing with results delivered via text in 5-6 hours. Taiwan, too, has tested every resident with unexplained flu-like symptoms for COVID-19 since January 31, 2020, and tests every traveler with fever or respiratory symptoms. Taiwan has had only one death from COVID-19 so far. Moreover, in addition to proactive testing, the government acted swiftly with crisis management tools, combatted misinformation, and focused on resource management throughout. We can see from Italy what happens when we don’t take a preemptive, wide-reaching approach. Let’s not squander the horrifying lesson they taught us. It’s clear that the US does not have the capacity to test at high levels like South Korea, meaning many people who are otherwise asymptomatic could be infecting the vulnerable classes in society. It took me many days to write this article because I can only stand for small 20-minute increments to write it with my CSF leak. But it’s well worth the “up time” if it makes a few more people take COVID-19 seriously. Stay home. Do what you can to protect the at-risk population. Change your schedule, your patterns, your habits to the maximum extent you can. Just because I’m vulnerable to this virus doesn’t mean I’m less worthy of staying well.
COVID-19 Resources
The post I’m In The Vulnerable Class for COVID-19. A Plea To Take This Virus Seriously. appeared first on Legal Nomads.       |
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/19782405/Coronavirus_Symptoms___WHO_joint_mission_2.png)


| You are subscribed to email updates from Legal Nomads. To stop receiving these emails, you may unsubscribe now. | Email delivery powered by Google |
| Google, 1600 Amphitheatre Parkway, Mountain View, CA 94043, United States | |



No comments:
Post a Comment